Limitations and Measurement Problems
The Bongaarts proximate determinants framework is theoretically strong. However, there are several limitations.
While Bongaarts’ framework on proximate determinants of fertility elucidates the relationship between level of fertility and biological and behavioural factors, it is of course a simplification of reality. As mentioned earlier, it is not intended to obtain an accurate estimate of total fertility rate. Rather, it is intended to aid the analysis and explanation of fertility differentials, by focusing interest on the links between each of the proximate fertility variables and various socio-economic and cultural ‘background’ factors. Several studies have attempted to apply the model using individual data, but it is often reported that the model does not explain all the variations in level of fertility due to some of the above reasons or due to the model itself. However, Baschieri and Hinde (2007) recently applied the model to explain the variations in birth intervals between the first and second children using individual’s contraceptive calendar data from an Egyptian Demographic and Health Survey (DHS).
Furthermore, It is worth noting that the framework was developed in the 1970s when individual demographic data were scarce, and some of the data, such as the data on abortion, effectiveness of contraceptive use and sexual activities, are hard to obtain accurately. Thus, a number of additional factors/complications are worth highlighting and may warrant consideration in certain circumstances.
1. Pathological sterility
While sterility was identified as one of the seven important proximate determinants, it was not included in the initial Bongaarts’ model. Pathological sterility, however, was responsible for large differentials in levels of fertility in sub-Saharan Africa. Based on the DHS data from 1995-2000, sub-Saharan Africa contained the countries with the highest proportion of childless women aged 40-44 (7.3 % in Cameroon, and, 10.5 % in the Central African Republic)(Rutstein and Shah 2004).
There are also practical measurement problems in determining infecundity. It is difficult to measure exposure to the risk of pregnancy over a period of years. In order to measure the exposure thoroughly, data on marital status, partner’s presence, abstinence, coital frequency and timing, contraceptive use and effectiveness (and its consistency of use) for all women of reproductive age for the entire period of interest are required. However, this information is difficult to obtain accurately.
2. Abortion
Abortion is one of the most difficult health issues to quantify. The estimation is particularly so in countries where abortion is illegal. Although abortion is not negligible and the rates vary across countries and over time, more data have become available and the estimation methods have been developed, it is still impossible to obtain reasonable total abortion rate (the number of abortions over the reproductive period per woman) for Bongaarts’ proximate determinants analysis. Therefore, most papers have assumed Ca is 1 (Rutstein 2002).
3. Exposure to pregnancy
3.1. Exposure to pregnancy outside marriage
In Bongaarts' model, sexual activities are considered to be confined within marriage. Prevalence of extramarital sex varies from country to country. One study reported less than 10% in Togo and Burundi up to over 15% in Tanzania (Caraël 1995). In developed countries, having multiple partners have been observed while it is more common among men globally (Welllings et al. 2006).
Extramarital births are found in many parts of the world.
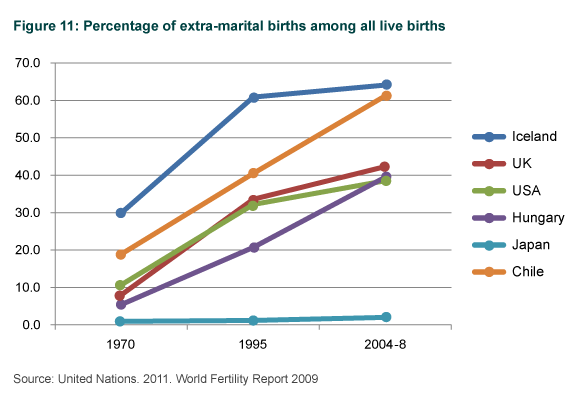
This shows changes in % of extra-marital births among live births. All the countries changed substantially in the last four decades with exception of Japan. Especially in Chile, proportion of births within marriage halved from 80% to 40%.
3.2. Exposure to pregnancy within marriage
Exposure to pregnancy within marriage or sexual union, that is, frequency of sexual intercourse, varies across populations, while the proximate determinants model assumed the coital frequency are similar across different populations. The WHO surveys on HIV/AIDS and sexual behaviour reported that proportions of currently married women aged 15-49 who had sex in the last month ranged from 42 % in Togo to 64 % in Tanzania (Caraël 1995). In other regions, such as Singapore and Thailand, the figure was more than 80 %. The mean coital frequencies in the last month prior to the survey were surprisingly as low as two or less in Togo, Côte d’Ivoire and Lesotho; whereas the mean in Rio de Janeiro was more than seven. In the same study in Europe, the means were between 6.8 and 8.4 episodes per month (Sandfort et al. 1998).
Furthermore, spousal separation may play a role especially in the population where economic migration is prevalent. Therefore, it is noteworthy that coital frequency varies across population.
*The data on sexual activities among unmarried and married are available in Demographic and Health Surveys (DHS) and Multiple Indicator Cluster Surveys (MICS).
4. Effectiveness of contraceptives
As mentioned earlier, it is difficult to measure the effectiveness of contraceptives. The use-effectiveness is calculated from number of unintended pregnancies by method. In order to measure the exposure to pregnancy thoroughly, data on marital status, partner’s presence, abstinence, coital frequency and timing for all women of reproductive age for the entire period of interest are required. Furthermore, stopping or switching the contraceptive methods is common. Thus it is difficult to measure the consistent use of contraceptive method over time.
5. Contraceptive prevalence
5.1. Overlap between contraceptive use and permanent infecundity
The model assumes that only fecund women use contraceptives. This assumption is reasonable in most cases. However, in some settings, a good number of women may have undergone sterilisation in countries where sterilisation is the primary method of family planning, such as in India. In these cases, some sterilised women were not fecund anyway.
5.2. Overlap between contraceptive use and postpartum amenorrhea
While the overlap between contraceptive use and postpartum amenorrhea generally seems modest, there is evidence that ‘double-protection’ is common in Zimbabwe.